The 'My Health Record View' tab
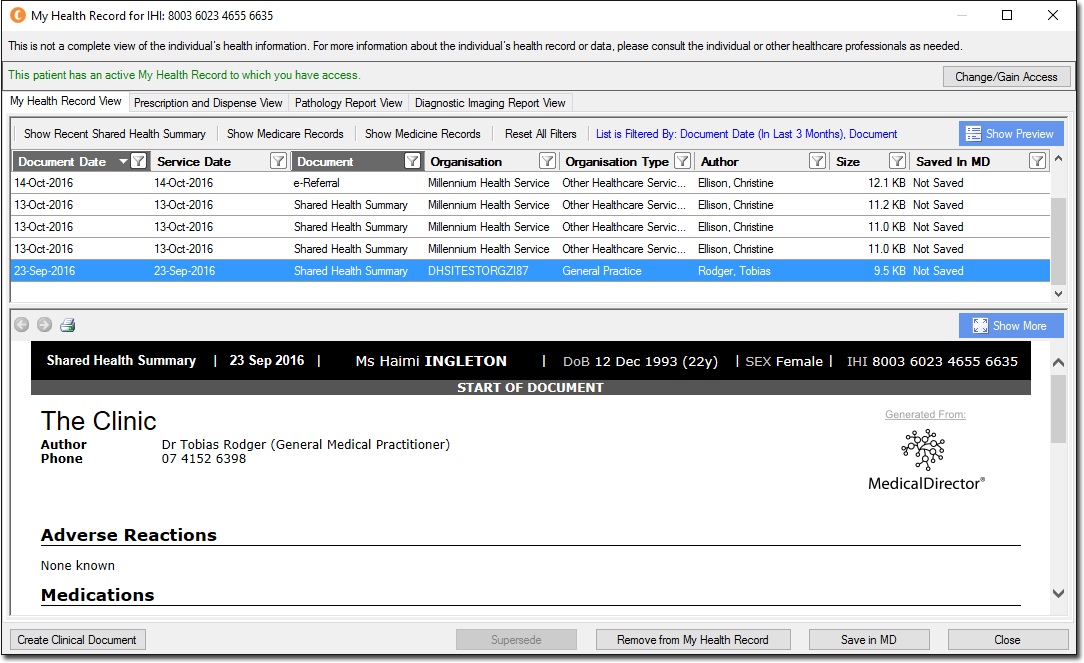
| The My Health Record View tab lists the patient's My Health Record documents. | |
 |
Allows you to gain access to documents that have been password-protected by the patient - it is the patient who controls access to their My Health Record documentation. Any document can be applied one of two access levels; Open: the document is unrestricted. Code: the document requires an access code to view/download. Click the Change/Gain Access button, and then select from the three Access Type options; Open Access: no access code required. Access Code: enables the Access Code field in which you must enter the access code the patient provided you. Emergency: grants you access to password-restricted documents for five days. To be used in an emergency when the patient cannot be contacted. A record of the document being accessed in this fashion may be sent to the patient. 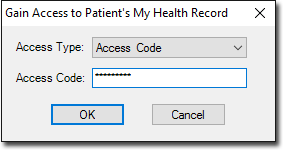 |
| Button: Show Recent Shared Health Summary | Displays the latest Shared Health Summary. This item will be disabled if there are no Shared Health Summaries to view. See Creating CDA e-Health Documents for information on creating Shared Health Summaries. |
| Button: Show Medicare Records | Retrieves MBS, PBS, AIR and ADOR records from the My Health Record System for the selected patient. |
| Button: Show Medicine Records | Retrieves prescription and dispensed records from the My Health Record System for the selected patient. |
| Button: Reset All Filters | Resets all filters applied to this tab. See Filtering Records on the My Health Record Window for more information. |
  |
Hides/shows the document preview pane in the lower half of the My Health Record window. |
| Navigate forward/backward through each page of a multi-page document. If a document consist of only one page, these buttons will be unavailable. | |
| Prints the selected document. | |
 |
Displays a selected document in Full Preview mode. |
 |
Closes 'Full Preview' mode, and display the list of documents again. |
 |
Opens Letter Writer and presents you with the New dialogue window, prompting you to select a new CDA eHealth document to create. |
 |
Replaces a selected document with a more recent version from the patient's record. The two documents must be of the same CDA type. |
 |
Removes a selected document from the My Health Record system. This is only available if you are the creator of the original document, or it was created by another user from the same Practice (i.e. with the same Practice HPI-O recorded via Tools > Options > Practice tab. |
 |
Saves a selected document to the patient's record in Clinical. The saved document will be available on the Documents tab within the Clinical Window, or the Letters tab in the case of a letter. |